Faith Carlson, a Clinical Therapist specializing in eating disorder treatment at Victus Counseling, was drawn to the field after learning that eating disorders have the highest mortality rate of any mental health condition, second only to opioid use disorder. She wanted to make a difference in helping those struggling with this life-threatening illness. As the only certified provider in South Dakota, Carlson frequently faces barriers that limit her ability to provide effective treatment, particularly with insurance-covered care, including fewer treatment options, denials, delays, and burdensome preauthorization requirements.
Carlson deeply understands the importance of access to mental health services and is acutely aware of the challenges and urgency individuals face when seeking help. After losing her brother, Andrew, to suicide in 2023, her commitment to advocating for mental health care grew even stronger. “People — brothers, sisters, children — are passing away from mental health illnesses. When access to services and barriers exist to getting care, lives are impacted. It has a real human life cost,” she said.
“When access to services and barriers exist to getting care, lives are impacted.”
Carlson’s patients face significant barriers, including opaque and sometimes unfair insurance restrictions, leaving them overwhelmed and at risk about if their care will be covered or if they’ll be paying out-of-pocket. As she explains, “This puts people in crisis. They already feel overwhelmed, they’re struggling to survive day-to-day, let alone trying to figure out who to call on the insurance end.”
The consequences can be fatal. One of Carlson’s first patients tragically died after being dropped from insurance and unable to secure the care needed. “It was such a devastation for me. I was doing everything I could to stabilize and support this client, but the reality was that there weren’t resources available,” Carlson explains. “These clients are passing away.”
“These clients are passing away.”
Nearly 1 in 10 Americans will experience an eating disorder in their lifetime, impacting millions. Carlson has a growing waitlist, with patients willing to travel long distances to see the only certified specialist in the area. Unfortunately, workforce shortages for behavioral health professionals are expected to worsen, and a lack of mental health parity enforcement can exacerbate the issue. As Carlson notes, “For one therapy hour, it’s two to three hours’ worth of work that’s not paid,” leaving her with a wage that is not livable.
“For one therapy hour, it’s two to three hours’ worth of work that’s not paid.”
Carlson underscores that investing in treatment on the front end can prevent costlier care, such as emergency room visits or inpatient treatment. “We need to keep people in their families, schools, and communities,” she said. “Parity enforcement would allow me to focus on my clients, helping them improve, function in society, and be the best versions of themselves.”
In her final thoughts, Carlson emphasizes the profound impact that proper support and care can have on individuals, families, and entire communities. “The work we do is critical, and with the right resources, we can help individuals not only survive but thrive.”
Voices in Parity highlights the real people experiencing mental health parity issues. Are you a person seeking mental health treatment who was denied care, or a provider dealing with mental health parity issues? Email in**@*************um.org to tell your story.
https://victusrecovery.com/wp-content/uploads/2025/06/IMG_0586-1.jpeg356422Victus Counselinghttps://victusrecovery.com/wp-content/uploads/2024/09/Logo_VictusCounseling.pngVictus Counseling2025-05-16 05:41:022025-06-03 05:42:59“Lives Are Impacted”: Therapist Battles Insurance Denials, Delays, and Hurdles That Affect Patient Care
For people in rural America, finding treatment for eating disorders is nearly impossible. Nearly 20% of patients live in states with no residential treatment in their state.
Geography doesnʻt seem like it should play a role in the landscape of eating disorders treatment, but in fact families and patients seeking rural mental health in small towns and cities and less populated states have far less recourse when it comes to treatment options than those on the east and west coasts and big cities in between — especially when it comes to eating disorders.
Thatʻs the reality Sioux Falls, South Dakota, residents Todd and Kimberly Peterson faced in 2019 trying to get help for their daughter Brittany, who was diagnosed with anorexia at 13. (MindSite News has changed their names to protect their confidentiality at their request.)
“Sioux Falls has about 250,000 people, and at that time there was just one person we could find that was seeing patients with eating disorder issues,” Todd said. Working with that therapist, they put a family-based treatment plan into action, but Brittany lost weight rapidly over the next few months.
“At that point, the therapist recommended doing inpatient hospitalization or residential treatment, and she was pretty serious about it,” said Todd. “She said if we don’t do this, she was afraid Brittany might not make it through.”
That was when the Petersons discovered that there wasnʻt a single residential treatment center in the entire state. After an extended search, they found a placement in Chicago, a nine-hour drive away. The distance became even more problematic when Brittany was stepped down to partial hospitalization (PHP), requiring Kimberly to take a leave of absence and find an apartment in Chicago while Todd remained in Sioux Falls caring for the coupleʻs other two children.
“What a hard time of life to be completely isolated only because you don’t have treatment in your own hometown,” Kimberly said “She was so young to be so far from home. It was really hard on her.”
“It’s a tragedy how we’re not serving our farmers, our rural communities.”
—FAITH CARLSON, THERAPIST AND EATING DISORDER SPECIALIST
The dearth of local treatment options again came into play again when Brittany completed outpatient treatment and returned home four months later.
“She was still actively battling her eating disorder all of that next year and she didn’t have a group that she could go to here, whereas in Chicago she had gotten so much peace and comfort from having other girls who knew what she was going through,” said Kimberly. “And we as parents had no support group.”
Cheri Levinson, director of the EAT Lab and clinic founder of the the Louisville Center for Eating Disorders. Photo: Natosha Via
Desperately seeking rural mental health services
Research conducted by the EAT Lab at the University of Louisville and Project HEAL shows that the Pettersonsʻ experience is not uncommon. A survey of eating disorder patients between January 2021 and June 2022 found that 34% of eating disorder patients were unable to find a treatment provider nearby, while 19% had no treatment centers available in-state. It’s even harder for patients insured through Medicaid.
“In Kentucky, if you have Medicaid, you are just out of luck. There are no residential centers or inpatient centers in the country that will take Kentucky Medicaid,” said Cheri Levinson, director of the EAT Lab and a founder of the Louisville Center for Eating Disorders.
Her clinic provides intensive outpatient and partial hospital programming but not inpatient. “When I have adolescents who need residential (care) and they’re on Kentucky Medicaid, I have literally nowhere that I can send them in the entire United States,” Levinson said.
“It’s a tragedy how we’re not serving our farmers, our rural communities,” said Faith Carlson, who became Brittany’s therapist and then opened her own disorders treatment practice, Victus Recovery, in Sioux Falls.
Eating disorder therapist Faith Carlson is concerned about the lack of services in rural America. Photo provided
With a background in nonprofits and community clinics, Carlson was determined to take Medicare and Medicaid when she set up her clinic. “Our Native American populations on our reservations have zero coverage, none. Thereʻs nobody helping, no access to resources. This is an untouched population and it’s alarming.”
“I went through the process of becoming approved, and then I submitted the claims for six months, and not one of my claims got reimbursed,” she said. “I wasn’t going to send these patients to collections. I wasn’t going to ask for money from people who are already struggling. So I had to make the very hard decision to stop accepting public insurance in order to build my business and keep the clinic open.”
In a written statement, Chris Bond, a spokesperson for America’s Health Insurance Plans (AHIP), an insurance trade association, noted that health plans follow the latest guidelines on reimbursement.
“Data on denials rarely take into account the overwhelming number of claims that are submitted from doctors that have extensive gaps in the accuracy and completeness of information provided, meaning health plans are regularly having to follow up to confirm correct billing and diagnostic codes” as well as proper treatment, he wrote.
In addition, Bond wrote that states, employers, and federal regulators “ultimately have an outsized and often final say on what benefits are included for consumers…Every aspect of insurance is regulated or reviewed by state insurance commissioners and federal regulators.”
Select References
Penwell TE, Bedard SP, Eyre R, Levinson CA. Eating Disorder Treatment Access in the United States: Perceived Inequities Among Treatment Seekers. Psychiatric Services. 2024;75(10):944-952.doi:10.1176/appi.ps.20230193
Timothy Walsh et al, A Systematic Review Comparing Atypical Anorexia Nervosa and Anorexia Nervosa, International Journal of Eating Disorders, August 2022
Bowman Family Foundation, Equitable Access to Mental Health and Substance Use Care: An Urgent Need, a Patient Experience Survey, July 2023, Conducted by NORC, University of Chicago
RTI International, Behavioral Health Parity – Pervasive Disparities in Access to In-Network Care Continue, Tami Mark, William Parish, April 17, 2024
Disparities in Access to Eating Disorders Treatment for Publicly-Insured Youth and Youth of Color, a Retrospective Cohort Study, Marissa Raymond-Flesch, UCSF corresponding author Ruby Moreno, Sara Buckelew et al, Journal of Eating Disorders, 2023
https://victusrecovery.com/wp-content/uploads/2025/05/brian-kelly-ln2GDpUzY-Y-unsplash-1024x683-1.jpg6831024Victus Counselinghttps://victusrecovery.com/wp-content/uploads/2024/09/Logo_VictusCounseling.pngVictus Counseling2025-05-15 04:47:222025-06-03 05:24:32‘We’re Not Serving Our Rural Communities’: One Eating Disorder Specialist for 250,000 People
For years, the media image of an anorexic youth was an emaciated white female teen. The stereotype was so pervasive that eating disorder specialists have an acronym for it: SWAG, or skinny, white, affluent girl.
For years, the media image of an anorexic youth was an emaciated white female teen.
One of the biggest barriers that keeps people with eating disorders from getting help is a cultural stereotype so pervasive that eating disorder specialists have an acronym for it: SWAG, or skinny, white, affluent girl. But studies show that anorexia strikes people of all races at approximately equal rates, and bulimia is actually more common among Latinos and African Americans.
“Eating disorders do not discriminate,” says Christine Peat, associate professor at University of North Carolina Chapel Hill and director of the National Center of Excellence for Eating Disorders (NCEED). “Although there is still this predominant stereotype of the skinny, white, rich girl, it just isn’t reflective of the patients that we’re seeing.”
“Eating disorders don’t discriminate,” says Dr. Christine Peat, director of the National Center of Excellence for Eating Disorders. Photo provided.
The problem is compounded by the fact that Black women in particular are nearly twice as likely as other groups to experience binge eating disorder, which tends to be taken less seriously than anorexia or bulimia but can have serious health impacts.Recent studies have also found that transgender youth experience anorexia, bulimia, and binge eating disorders at two to four times the rates for cisgender youth.
The general view of a person with an eating disorder is “somebody who is not just underweight but really at death’s door, (which is) such a small percentage of people with these conditions,” Peat said. “The vast majority of patients are not going to have frank signs or symptoms of an eating disorder. They are actually going to be well within normal or even elevated limits when it comes to BMI.”
This changed understanding is reflected in the rise of a relatively new diagnosis, atypical anorexia nervosa, which appears in people who are not clinically underweight. This sub-diagnosis was added to the DSM-5 in 2013 and in the decade since has accounted for a rapidly growing percentage of those with eating disorders. A growing body of research shows that people with atypical anorexia suffer effects just as serious as those with regular anorexia.
“There are all kinds of health and medical complications that you can have with atypical anorexia nervosa,” Peat said.
These misconceptions – and the resulting failure to identify and treat anorexia, bulimia, and other eating disorders – fuel a dangerous tendency to overlook and underdiagnose eating disorders in those who don’t fit the prevailing image.
“Because people don’t present as what we think of stereotypical patients for eating disorders, they’re just getting missed completely,” said Doreen Marshall, CEO of NEDA. “And then because you’re getting missed, I think it reinforces the idea that treatment’s not for me – or is too hard for me to access.” In addition, doctors are significantly less likely to ask their BIPOC patients about eating and weight concerns than their white patients.
Getting out the message that eating disorders don’t discriminate
Changing the public perception of who suffers from eating disorders is the mission of the Eating Disorders Information and Training Network, a web-based education and training program. The project aims to provide education and training for eating disorders diagnosis and treatment aimed at both the public and at physicians and other health care practitioners.
“The vast majority of physicians don’t receive any training on eating disorders or if they do, it’s maybe a lecture or two and that information may be really outdated,” Peat said. “Most mental health folks actually aren’t trained in eating disorders, either. They might be more familiar with some of the diagnostic criteria because it’s part of learning the DSM, but that doesn’t mean they’re equipped to actually do the care.”
To this end, the National Center for Excellence for Eating Disorders has developed a streamlined, web-based diagnostic tool for primary care practitioners: SBIRT-ED, which stands for Screening, Brief Intervention, and Referral to Treatment for Eating Disorders. The methodology is based on a similar screening tool developed for substance use disorders, depression and anxiety.
“If this is a framework that works, we don’t need to reinvent the wheel,” Peat said. “Maybe if we catch people earlier in their disease progression, for example, at an annual wellness visit, they may not ever need to see a specialist like myself but instead can take advantage of other less intensive kinds of care. Part of what weʻre trying to do is increase the capacity of the entire health care workforce to engage in this kind of care.”
Uncaptioned photos above licensed from Shutterstock.
Select References
Penwell TE, Bedard SP, Eyre R, Levinson CA. Eating Disorder Treatment Access in the United States: Perceived Inequities Among Treatment Seekers. Psychiatric Services. 2024;75(10):944-952.doi:10.1176/appi.ps.20230193
Timothy Walsh et al, A Systematic Review Comparing Atypical Anorexia Nervosa and Anorexia Nervosa, International Journal of Eating Disorders, August 2022
Bowman Family Foundation, Equitable Access to Mental Health and Substance Use Care: An Urgent Need, a Patient Experience Survey, July 2023, Conducted by NORC, University of Chicago
RTI International, Behavioral Health Parity – Pervasive Disparities in Access to In-Network Care Continue, Tami Mark, William Parish, April 17, 2024
Disparities in Access to Eating Disorders Treatment for Publicly-Insured Youth and Youth of Color, a Retrospective Cohort Study, Marissa Raymond-Flesch, UCSF corresponding author Ruby Moreno, Sara Buckelew et al, Journal of Eating Disorders, 2023
https://victusrecovery.com/wp-content/uploads/2025/05/shutterstock_2487808491.jpg6671000Victus Counselinghttps://victusrecovery.com/wp-content/uploads/2024/09/Logo_VictusCounseling.pngVictus Counseling2025-05-14 04:42:122025-06-03 05:22:26Eating Disorders: They Don’t Just Happen to Skinny, White, Affluent Girls
Across the country, a small group of lawyers and care navigators help patients, often desperately ill, battle with health insurers to access services. It’s a high-stress job, and “you don’t save everybody.”
The barriers to eating disorder treatment are depressingly familiar to Alexa Grayson and her team at Project HEAL. The mission of the Parkville, Maryland, nonprofit is to break down the barriers that keep people with eating disorders from getting treatment — and the insurance coverage that will pay for it. The program helps people negotiate with programs and insurers and it sometimes functions as a last resort, a place where people who canʻt get help in other ways can apply for short-term treatment grants.
Project HEALʻs navigators often guide people through the process of applying for a so-called single-case agreement to obtain insurance coverage for an out-of-network provider. Getting one is far from easy, however. To qualify, people must prove that the service they need is not available in-network due to lack of qualified providers or treatment programs.
Alexa Grayson is the insurance navigation program manager at Project HEAL. Photo provided.
“This is not something insurance loves to willingly share,” said Grayson, who manages the insurance navigation program. “If you call member services, a lot of them probably don’t even know what a single-case agreement is, especially one that’s eating disorder-specific. There are a lot of specific steps you have to take.”
Demand is rising rapidly. Two years ago, Grayson said, Project HEAL was receiving fewer than 20 applications for assistance a month. Today, the number often exceeds 80.
Delays in getting treatment approved can be deadly, especially for those with severe anorexia and bulimia. Often, Grayson said, it has to get to the point that someoneʻs symptoms are severe enough to cause serious physical damage requiring hospitalization before coverage kicks in. For those in an earlier stage of the disorder, delaying treatment or receiving a lower level of care than needed can prolong the disease and allow it to progress.
“Thatʻs part of why our system is so overwhelmingly broken,” Grayson said.
In dozens of interviews, families, attorneys and eating disorder advocates detailed the extensive barriers they faced that blocked or delayed the start of treatment. Even when they get the OK from an insurance company to begin therapy, patients often find few or no in-network providers with expertise in treating eating disorders. And then, if they’re lucky enough to find an appropriate clinician, that provider is likely to be fully booked with a long waiting list.
“What insurance companies fail to appreciate is that it takes a long time for the brain to heal; it has to develop new pathways, the patient has to overcome their fear of eating.”
—TRISHA WESTMORELAND, MEDICAL DIRECTOR, ACUTE CLINIC IN DENVER
Even when doctors recommend higher levels of care – such as intensive outpatient treatment, partial or full hospitalization or residential treatment – families often find that the nearest facility is in another state, hundreds or thousands of miles away, that insurers will only approve lower, less expensive levels of care and that they must be prepared to pay hefty out-of-pocket costs. But some nonprofit health groups are trying to bridge the gap.
“What the insurance companies fail to appreciate is that it takes a long time for the brain to heal; it has to develop new pathways, the patient has to overcome their fear of eating,” said Trisha Westmoreland, medical director for the ACUTE clinic in Denver. “Patients and families are put in a very difficult position when they arenʻt given enough time. It becomes this revolving door and that wouldnʻt have happened if theyʻd had an adequate course of treatment the first time.”
Westmoreland notes that ACUTE has less difficulty getting insurance coverage when patients are medically unstable. “Once people step into the behavioral health realm, itʻs very difficult to document that they need more time in a supervised setting,” she said. “People donʻt understand the severity. They donʻt realize that anorexic patients can die with stone cold normal lab results. Or that no matter what weight a patient is at, if they purge frequently enough they can drop their potassium really quickly, and they can have a seizure or cardiac arrhythmia and they can die.”
“There are people we know and have cared for, for years. They may have come back a few times – and then we will hear from former patients or other providers that they died,” she said. “It’s so incredibly sad because we obviously work really hard with these patients and there is always the potential to help people get better. But you don’t save everybody.”
Danielle Ellis. Photo provided
The experience of Danielle Ellis is a perfect illustration of this frustrating cycle. A high school and college athlete who played three different sports, Ellis began severely limiting her food intake and over-exercising in high school, following the example of her mother, who also had an eating disorder. But it wasn’t until she was in her first years of college that the disease took control and her weight declined precipitously. She was diagnosed with anorexia at 21, and has been in and out of outpatient and residential treatment ever since, including three different hospital stays at ACUTE in Denver.
Ellis, now 32 and a school therapist in Georgia, says she was often caught between being too sick for outpatient residential treatment and not sick enough to be in the hospital. When she was hospitalized, Ellis recounts, she was often discharged without adequate follow-up support, and ended up relapsing. At those places, “it feels like they donʻt care about you,” she says. “Like they’ve given up on you.”
Ghost networks and a broken system
One way insurance companies limit care is by requiring patients to get treatment only from a list of approved providers – the “network.” When there are few providers on the list, patients are forced to go “out-of-network” – and pay much or all of the provider’s fee. Small networks limit access to all types of mental health care: According to a recent report from the Bowman Family Foundation, 39% of patients in employer-sponsored health plans used at least one out-of-network mental health or substance use provider for outpatient care, compared to 15% for physical health providers..
Studies have also documented the growing use of what researchers call “ghost networks” – listings of providers who do not actually practice, take new patients or even exist. Some reports have found practitioners listed in insurance networks who are retired or dead.
When insurers have small networks, patients – who often are in dire condition – or their families are forced to spend time trying to find a covered practitioner. The Bowman report found that 40% of insured patients had to contact four or more providers to find an in-network provider for outpatient mental health or substance use care compared with only 14% of those seeking a physical health care provider.
Health plans and insurers mentioned in this series, including Cigna, Anthem, and Blue Cross/ Blue Shield, did not respond to requests for comment from MindSite News. UnitedHealthcare responded but declined to comment.
In a written statement, Chris Bond, a spokesperson for America’s Health Insurance Plans (AHIP), an insurance trade association, noted that health plans’ coverage decisions “follow the latest medical guidelines on treatments and medical care that are proven to be safe and effective. Data on denials rarely take into account the overwhelming number of claims that are submitted from doctors that have extensive gaps in the accuracy and completeness of information provided, meaning health plans are regularly having to follow up to confirm correct billing and diagnostic codes” as well as proper treatment.
In addition, Bond wrote that states, employers, and federal regulators “ultimately have an outsized and often final say on what benefits are included for consumers. So if a service is not included as part of coverage – as a result of an employer’s coverage policy or a state requirement – then it’s important to understand that distinction.” Finally, he added, “every aspect of insurance is regulated or reviewed by state insurance commissioners and federal regulators.”
The problem is that patients can get lost or swallowed up in the process, advocates say.
“If people spend all this time and can’t find a qualified therapist or can’t find treatment they can afford, sometimes they just give up. And that means someone goes untreated,” said therapist Lauren Muhlheim. Her Los Angeles-based practice specializes in eating disorders and accepts insurance – including Medicaid and Medicare – as an in-network provider.
Since insurance networks offer therapists reimbursement rates that are often just 50% of the going private rates, providers have little incentive to join, Muhlheim said. The RTI report backs this up, showing that the average reimbursement rate for office visits to behavioral health clinicians was nearly 22% lower than to medical providers.
And if accepting low fees wasn’t bad enough, Mulheim said, she also must pay office workers to handle the huge amounts of paperwork required by insurers.
“I have nine therapists, and I have three admin personnel just to handle the paperwork,” Muhlheim said. “You’ve got to be a certain size for it to be practical and thatʻs just not possible for most sole providers or small groups.”
Provider networks can also be deceiving: A search for “eating disorders” in a network directory may turn up available therapists, but those listed may have little or no experience treating eating disorders. Mulheim says that’s because therapists applying to be included on an insurer’s “panel” of practitioners are given a list of as many as 40 different areas of speciality.
“A lot of the insurance companies don’t really vet, they just tell you to check all the things you treat,” Muhlheim said. “People want to be chosen for the panel so they think they should just check as many things as they can, but they donʻt actually have any experience.”
The impact of private equity
One force affecting the availability of inpatient care has been the growing ownership of eating disorder treatment facilities by private equity firms. Observers say these firms typically operate by pouring resources into companies and expanding them to make them attractive to other investors while also cutting costs, before ultimately cashing out in a sale.
“Their model is to expand and open up multiple sites, and then look for an exit,” said Ethan LeFever, director of ViaMar Health in Florida, an eating disorders treatment facility that is privately owned by his family.
But with profit as investors’ primary driver, treatment centers owned by private equity firms are under pressure to cut costs. “They’re selling at these huge multiples, which means they have to take all this profit out of it,” Muhlheim said. “This is most easily accomplished by increasing patient-to-staff ratios and in some cases replacing long-time, experienced staff with newer hires.” This often means losing “extras” like art therapy, support groups, and more.
“When facilities were smaller and privately run and those folks were involved intimately with their own center and their vision and purpose, the care translated to being better and more individualized,” LeFever said. “You had a lot more attention to the human on the other end because you’ve got clinicians with their boots on the ground who were involved in the care that their name was on.”
“In Kentucky, if you have Medicaid, you are just out of luck: There are no residential centers or inpatient centers in the country that will take Kentucky Medicaid.”
—CHERI LEVINSON, DIRECTOR OF THE EAT LAB AT THE UNIVERSITY OF LOUISVILLE
Observers say there’s another problem, too: Very few private equity-owned residential facilities that treat eating disorders accept public insurance. That means that patients who are covered by Medicaid are essentially excluded from these programs, making it extremely difficult for low-income patients and patients of color to find residential programs that serve them.
The kitchen of the Louisville Center for Eating Disorders is equipped with lockers, comfortable seating and affirmations to support patients on a journey to healing. Photo: Natosha Via
“In Kentucky, if you have Medicaid, you are just out of luck: There are no residential centers or inpatient centers in the country that will take Kentucky Medicaid,” said Cheri Levinson, director of the EAT Lab at the University of Louisville, whose clinic provides intensive outpatient and partial hospital programming but not inpatient. “When I have adolescents who need residential (care) and they’re on Kentucky Medicaid, I have literally nowhere that I can send them in the entire United States.”
With fewer services and a smaller, less experienced staff, private equity firms “have reaped financial gain at the expense of their food-challenged, largely female patients,” wrote Laura Katz Olson, distinguished professor of political science at Lehigh University in her 2022 book, Ethically Challenged: Private Equity Storms US Health Care.
Those who need a higher level of care frequently can’t get into for-profit treatment programs that won’t accept Medicare and Medicaid and must rely instead on university-based programs that take insurance, said Jennifer Wildes, a professor of psychiatry and neuroscience and director of the Eating Disorders Program at University of Chicago. But many such programs, including hers, are outpatient only, providing family-based treatment and cognitive behavioral therapy to children and adults, with medical consultation provided by the medical centerʻs doctors.
“The real challenges tend to come for our folks with Medicare and Medicaid if we need to step them up to a higher level of care,” Wildes said. “We often find ourselves sort of stuck with these patients who really aren’t appropriate for our level of care, but don’t have any other options. Even our well-insured clients run up against very high deductibles and will have to pay a lot out of pocket before they hit that amount.”
“The treating doctors are saying, ‘She really needs to stay longer.’ And the insurance company is saying, ‘Well, our reviewer said she’s had enough.’”
—LOS ANGELES ATTORNEY LISA KANTOR
Private equity-owned behavioral health companies have a history of acquiring, then closing smaller eating disorder treatment centers. When Shoreline Center for Eating Disorder Treatment in Laguna Hills, California was acquired by Odyssey Behavioral Healthcare in 2021, Shoreline’s CEO Rachel* Levi said in a press release that “Odyssey and Shoreline make an ideal match and we’re thrilled to be joining their network of renowned eating disorder facilities.”
Two years later, Odyssey closed the Shoreline program, and in December 2024, Odyssey quietly sold to JLL Partners, another PE-backed behavioral health company. Levi, the former owner, contacted MindSite News by email in response to this story to express her disappointment with the closing of the program.
“What a slap in the face,” she wrote. “Their commitment to the programs was smoke and mirrors. Such a huge disappointment.”
An easy target for insurance companies
Attorneys who handle eating disorders cases have a front row seat to the desperation of families seeking treatment. “Eating disorders have become an easy target for insurance companies because they don’t want to pay for a lot of care, and eating disorders are complicated and difficult to treat,” said Hufford, who litigated a landmark parity case, Wit vs. United Behavioral Health. “They would like to try to treat issues quickly and then reduce the level of care.”
Some eating disorder patients manage to get their insurers to pay for a week or two of treatments before conflict sets in between doctors and insurance reviewers, said Los Angeles attorney Lisa Kantor, whose law firm represents people denied health benefits for treatment of eating disorders and other illnesses. “The treating doctors are saying, ‘She really needs to stay longer.’ And the insurance company is saying, ‘Well, our reviewer said she’s had enough.’” Yet terminating treatment prematurely can cause serious harm, Kantor said.
“If someone has cancer, you don’t treat them to 85% of recovery; you treat them until you think the cancer is gone,” she said. “But what we’re doing with eating disorders is we’re saying, ʻWell, we’ve gotten you to the point where you’re not actively trying to kill yourself, you’re not actively trying to hurt yourself, your weight is better, basically go home and do the rest on your own.ʻ”
“Itʻs insane,” Kantor added. “It doesn’t make any sense. I’ve had more clients die trying to get treatment than I want to remember. It’s an epidemic and a complete tragedy.”
“Iʻve had more clients die trying to get treatment than I want to remember. Itʻs an epidemic and a complete tragedy.”
—ATTORNEY LISA KANTOR
To Domna Antoniadis, the purpose of all these restrictions is clear: “The idea is to make it so difficult, people just give up,” she said.
Few advocates are as well-prepared to challenge such restrictions as Antoniadis, who has been both a plaintiff in a key class-action suit and a lawyer representing eating disorder patients. She was Jane Doe in the landmark Jane Doe v. United HealthCare that the giant insurer agreed to settle in 2021. The agreement required United to pay more than $18 million to settle allegations that the company violated patients’ right to mental health coverage under federal parity regulations.
“I did my first inpatient treatment in my early 20s, and that was actually the motivation for going to law school because I found out there were laws about this stuff,” said Antoniadis, who is now 39. “I was able to use them to fix things and I thought, ‘This is incredible.’”
Domna Antoniadis uses her experience with eating disorders to inform her work as an attorney. Photo provided.
Since then, she says, she has helped dozens of people get claims approved. She amassed a trove of records and submitted them as evidence to support rule changes proposed by the Biden administration to strengthen the parity law, including provisions that apply to Medicaid Those rules became final in October, three months before the end of Biden’s term. They may now become almost meaningless as the Trump administration decimates the federal workforce and Congress considers drastic cuts to Medicaid.
In part I of this series, Megan H. and Gigi T. were at a low point in their struggle with the severed anorexia. Danielle Ellis, who also suffered from anorexia, sometimes despaired of getting better. But despite all their obstacles, Megan, Gigi, and Danielle – three women with eating disorders – are all in recovery. Megan is back full time as a trauma nurse in San Diego, and Gigi is in college. Danielle Ellis is working with young students in Georgia. All are quick to say they are lucky.
“I have at least a dozen people I know that didnʻt make it,” Ellis told me. “And thatʻs scary to think about because that could have been me.”
They also say the struggles they went through with obtaining coverage for treatment prolonged their sickness. “When you’re getting all these letters from insurance companies denying care, it completely fuels the disease,” said Megan H. “Your family and friends are telling you you need help, but the insurance company is telling you that you’re not sick enough. And you internalize it as ‘Youʻre not deserving enough.’”
Danielle Ellis, who was eventually treated by a dedicated team of eating disorder specialists, puts it this way: “For a long time, I really didn’t care if I lived. But the doctors and staff cared, and that made me try even when I was ready to give up. Having people care and believe in you makes you believe in yourself. That’s what I wish everyone understood.”
*Note: This story has been updated to add Rachel Levi’s correct first name, which was misidentified due to an editing error, and to add her comments on the regrets she has in selling her treatment program to Odyssey Behavioral Health in 2021.
Select References
Penwell TE, Bedard SP, Eyre R, Levinson CA. Eating Disorder Treatment Access in the United States: Perceived Inequities Among Treatment Seekers. Psychiatric Services. 2024;75(10):944-952.doi:10.1176/appi.ps.20230193
Timothy Walsh et al, A Systematic Review Comparing Atypical Anorexia Nervosa and Anorexia Nervosa, International Journal of Eating Disorders, August 2022
Bowman Family Foundation, Equitable Access to Mental Health and Substance Use Care: An Urgent Need, a Patient Experience Survey, July 2023, Conducted by NORC, University of Chicago
RTI International, Behavioral Health Parity – Pervasive Disparities in Access to In-Network Care Continue, Tami Mark, William Parish, April 17, 2024
Disparities in Access to Eating Disorders Treatment for Publicly-Insured Youth and Youth of Color, a Retrospective Cohort Study, Marissa Raymond-Flesch, UCSF corresponding author Ruby Moreno, Sara Buckelew et al, Journal of Eating Disorders, 2023
https://victusrecovery.com/wp-content/uploads/2025/06/DSC09862-1024x683-1.jpg6831024Victus Counselinghttps://victusrecovery.com/wp-content/uploads/2024/09/Logo_VictusCounseling.pngVictus Counseling2025-05-13 05:08:342025-06-03 05:19:21‘A Front Row Seat to Desperation’: Meet the Advocates Fighting to Remove Barriers to Eating Disorder Treatment
Eating disorders are America’s deadliest mental health condition. For people struggling to get care, health insurers create some of the most formidable hurdles.
Part 1 of Deadly Denials, a four-part series supported by the Pulitzer Center.
The worst moment in Beth T’s life came on a Thursday afternoon in June 2020, when she got a call from McCallum Place, a residential treatment facility for eating disorders in St. Louis, Missouri. Beth’s daughter Gigi (a pseudonym) had spent five months there being treated for severe anorexia. Gigi, then 14, had refused food for weeks and was on a 24-hour feeding tube. Nonetheless, an official at McCallum Place told her, Gigi had to go home. “They said insurance is done and you have to pick her up tomorrow,” Beth recalls.
“I asked, ʻHow are my husband and I supposed to do the work of a five-person medical team here at our home?ʻ” said Beth. ”And they said, ʻWell, we don’t know, but insurance is quitting so you have to come.”
After multiple frantic calls, Beth managed to get a one-day extension. She describes what happened next: “They met us in the parking lot on Saturday morning with two Ziploc bags full of medications with labels on them and all these instructions on how we’re supposed to administer them to her. ʻHere are the ones that are about to run out – you’ll need a psychiatrist to get that done. These are the ones where she has some left.’”
In a stroke of luck, the family found an outpatient eating disorder specialist willing to take Gigi on despite the short notice. But to keep her safe at home, one parent had to be with her at all times, requiring Beth and her husband to take repeated leaves of absence, trading off week by week.
Sadly, the parents were all too familiar with the exhausting demands of caring for a child with an eating disorder – Gigi’s older sister had previously spent years in treatment for anorexia as well.
McCallum Place did not reply to repeated requests for comment.
Fortunately, Gigi got regular outpatient care and gradually improved over the next year. She was eventually able to return to school, as long as her parents closely supervised her with regular outpatient care and strict supervision during meal times. But the respite was short-lived. Gigi has been in and out of residential and partial hospitalization programs six more times, a revolving door her mother attributes in part to repeated delays, denials and premature step-downs by their insurance carriers.
“I’ve been with several different insurance companies and all of them are the same,” Beth said. “They only approve a week of residential treatment at a time. It’s just week to week and they can drop you from one day to the next.”
In many cases, she said, the treatment programs get so frustrated negotiating with the insurer for extensions that they discharge the patient. Even when claims are approved, they cover only part of the expense. Beth said her family has paid tens of thousands of dollars in out-of-pocket costs for Gigi’s treatment over the years, and one recent bill for seven months in a treatment program left them with $3,740 in out-of-pocket expenses.
The deadliest mental health disorder
Eating disorders are the deadliest of all mental health conditions (not including substance use disorders) and claim, on average, 10,200 lives a year, or one every 52 minutes, according to the National Association of Anorexia Nervosa and Associated Disorders. More than a fourth of people with an eating disorder attempt suicide. Rates have soared since the start of the pandemic in 2020, with eating disorders among teens more than doubling, the UMass Chan Medical School reports. A separate report found a 108% jump in the percentage of children treated for an eating disorder and a 131% increase in claims during the Covid pandemic.
Like Gigi’s parents, many families find themselves paying thousands of dollars in out-of-pocket fees. But the stress and anxiety from exorbitant bills pales in comparison to having treatment for an eating disorder denied outright.
“The battle to get my HMO to approve the treatment I needed was just insurmountable. I was so worn down, I said, ʻI’m done with this. I can’t do it anymore.ʻ”
—MEGAN H, PATIENT WITH SEVERE ANOREXIA
Two years ago, Megan H. left her job and her apartment and went home to spend her final days in hospice, supervised by a palliative care team. Down to 80 pounds on her 5’8” frame and medically unstable from the effects of severe anorexia, she was ready to give up. “I couldn’t even get down the stairs in my apartment. I couldnʻt shower,” she said. “The insurance battle trying to get my HMO to approve the treatment I needed was just insurmountable. I was so worn down, I said, ʻI’m done with this. It’s going to be the same cycle and I can’t do it anymore.ʻ”
It didnʻt have to be this way – there was a place waiting for her at the ACUTE clinic at Denver Health Medical Center, which specializes in treating eating disorder patients with serious medical issues such as malnutrition and cardiac instability. Megan had been treated at ACUTE once before, and achieved a period of recovery before the downward spiral began again. But this time, the insurance company deemed out-of-state treatment unnecessary and directed Megan to a local southern California psychiatric facility.
Attorney Domna Antoniadis has used her experience with eating disorders to inform her work as a legal advocate. Photo provided.
That facility had other ideas. “They said ‘Absolutely no way, she’s not medically stable, we’re not equipped to handle that,’” Megan recalled.
The catch-22 was nothing new for Megan, who first began restricting food and over-exercising as a junior in high school. Now 40 and an ICU nurse in San Diego, she’s spent more than half her life struggling with the disease. For the previous three years she had spent much of her time on a feeding tube, infusing herself through a port in her abdomen.
Megan’s medical team, however, refused to give up, reaching out to attorney Domna Antoniadis, a senior staff attorney at LegalHealth who has become a fierce advocate using knowledge and tactics she gained during her own battle for eating disorders coverage. Within days, the approval came through.
At that point Megan declined treatment: She was physically weak and had already accepted hospice care. But she rallied soon afterward and changed her mind.
“I was life-flighted to Denver, which saved my life,” Megan said. “But it was quite a fight to get there. And it was a very close call.”
Cheri Levinson, clinic founder (left), and Stacey Annis, director of operations, in front of the Louisville Center for Eating Disorders clinic in Louisville, Kentucky on Friday May 9, 2025. Photo: Natosha Via
Stories that are all too common
These stories from Megan H. and Beth T. are not outliers; they represent an all-too-common scenario faced by families and adults with eating disorders around the country. A 10-month investigation by MindSite News has found evidence that many health insurers and managed care organizations have pursued practices that limit care for eating disorders instead of meeting the growing need for services.
Insurers typically deny claims in one of two ways: They impose numerical limits in policies on the number of visits or days of coverage an insured patient can receive. Or,
more commonly, they issue denials based on their contention that a particular treatment is not medically necessary, requires prior authorization or must be preceded by a less intensive (and less expensive) treatment. These kinds of denials are known by a wonky term: non-quantitative treatment limitations (NQTLs).
Unpublished data reveals the barriers
Until recently, little hard data was available to document the impact of these restrictions, but that has changed. In 2021, the Eating Anxiety Treatment (EAT) Lab at the University of Louisville in Kentucky and Project HEAL, a nonprofit that helps people with eating disorders find services and seek insurance coverage, joined forces to survey eating disorder patients.
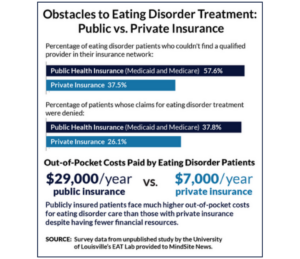
Unpublished data shared with MindSite News by researchers at the EAT Lab showed that people with both private and public insurance faced major obstacles getting treatment for eating disorders. But on nearly all metrics, publicly insured patients had a harder time getting services and coverage. Specifically, they found:
57.6% of those with public insurance said they were unable to access a qualified eating disorder provider in their insurance network, compared with 37.5% of those with private insurance.
37.8% of people with public insurance reported having claims for eating disorder services denied, compared with 26.1% of those with private insurance.
Those on public insurance, who are likely to be lower income, reported higher out-of-pocket costs, spending an average of $29,000 a year vs. an average of $7,000 for those with private insurance.
Survey: 96% of patients encounter obstacles to eating disorders treatment
A survey by the EAT Lab researchers, published last year in Psychiatry Online, reveals the barriers to treatment experienced by eating disorder patients, including the most common reasons insurers deny their claims:
43% of respondents reported that their insurer considered the requested level of care to be inappropriate
43% said theyʻd been discouraged from seeking treatment because they didnʻt seem sick enough
36% reported there were no eating disorder providers in their insurer’s network
30% reported they were prematurely discharged from the right level of care
26% reported that the level of care recommended by their clinicians was denied
23% reported that their insurer limited the number of visits
Overall, 96% of patients and their families reported encountering at least one barrier to accessing treatment. The most common: financial barriers, encountered by 81% of patients.
“It’s a nightmare,” said Dr. Cheri Levinson of the EAT Lab at the University of Louisville. “Insurance companies are dictating the care that you’re able to give patients. We would have patients who were super sick and insurance (companies) would, say, give them two weeks of treatment. And we would say they are not ready to leave after two weeks of treatment, and they would not care.”
As an example, she cited more than one patient who was discharged from the hospital when she gained enough weight to put her over a numerical threshold for Body Mass Index (BMI) specified by the company’s medical reviewer – but was then deemed too sick to be stepped down to intensive outpatient care, the next logical level of support.
“It’s like no matter what you did – if she gained weight or lost weight – they would just come up with a reason to not give any more days of treatment even though we, the eating disorder experts, are saying she needs more treatment,” Levinson said. “This is really detrimental for treatment progress because patients know ‘I only have three days of treatment,’ and then they get so stressed out that they can’t even focus.”
To further complicate Levinson’s work, she learned in late April that two grants to the EAT Lab were abruptly terminated by the National Institutes of Health, eliminating $289,000 in funding she uses to support the work of two clinical researchers. The grants, awarded last August and originally approved to run through August 2026, are among almost 800 NIH grants abruptly cancelled by the Trump administration, according to reporting by the journal Nature.
The offices of the Louisville Center for Eating Disorders, Friday May 9, 2025. Photo: Natosha Via
Bethany Schoch, administrative assistant, at Louisville Center for Eating Disorders. Photo: Natosha Via
“The supplemental award is terminated,” stated the NIH notice, because “research programs based primarily on artificial and non-scientific categories, including amorphous equity objectives, are antithetical to the scientific inquiry, do nothing to expand our knowledge of living systems, provide low returns on investment, and ultimately do not enhance health, lengthen life, or reduce illness.”
One of the EAT Lab grants pays the salary of a therapist who provides mental health treatment to eating disorder patients with serious medical complications. The other supports a PhD student who has been developing a machine learning algorithm that can help predict the likely development of eating disorders in children ages 8 to 12. Levinson said she will shift funding from other sources to cover the salary of the therapist and ensure continuity of care for existing patients, but the PhD student is halting his research and will have to work as a teaching assistant in order to complete his doctoral studies. “We won’t allow it to impact patient care,” she said. “But in the long term, it’s going to have an impact.”
The push for parity and equitable coverage
In a recent study published in the Journal of Eating Disorders, researchers compared treatment rates for youth ages 15 to 25 in an urban adolescent specialty program and found that those with public insurance were one third as likely as patients with private insurance to receive recommended treatment. The data also showed that Latino and Asian patients were only half as likely as white patients to get the recommended treatment.
The barriers encountered by people with eating disorders are part of a wider problem: Patients who need mental health services often struggle getting insurers to cover them, despite federal and state “parity” laws requiring equivalence in insurance coverage.
Despite these laws, a 2024 report by RTI International, a North Carolina-based research institute, found that patients went out of their insurance networks 8.9 times more often for psychiatrist office visits and 10.6 times more often for psychologist office visits than for medical visits – requiring them to pay more out-of-pocket in co-pays or to abstain from treatment.
For residential care – required for many eating disorder patients – the RTI data revealed even greater disparities, with mental health patients forced to go out-of-network 19.9 times more often for inpatient subacute care compared to patients seeking medical or surgical care in such facilities.
“Weʻve had patients that we essentially felt like we were sending home to die”
—CHERI LEVINSON, UNIVERSITY OF LOUISVILLE EAT LAB
And although parity laws apply to Medicaid, patients on the government-funded health insurance program face even more daunting obstacles, including, in some cases, a complete lack of higher-level care.
“In Kentucky, if you have Medicaid, you are just out of luck: There are no residential centers or inpatient centers in the country that will take Kentucky Medicaid,” said Levinson, whose clinic provides intensive outpatient and partial hospital programming but not inpatient. “When I have adolescents who need residential (care) and they’re on Kentucky Medicaid, I have literally nowhere that I can send them in the entire United States.”
“We’ve had patients that we’ve essentially felt we were sending home to die because there’s nothing that we can do to get them in somewhere,” she added. At times, faced with the prospect of turning patients away, Levinson said, she and her team provided care pro bono.
Many patients enter a revolving door, in which they no longer qualify for coverage of certain services because their body-mass index (BMI), electrolyte levels, malnutrition or menstruation patterns improve slightly – even though such metrics may have little bearing on whether they’re adequately recovered from a psychological standpoint. Without adequate support, their condition then deteriorates until they are once again sick enough to require hospitalization or inpatient treatment.
A recent staff photo of the University of Louisville EAT Lab, which was recently notified that two federal grants had been cancelled by the Trump administration, eliminating $289,000 in research funds. Photo courtesy of the EAT Lab
Health plans and insurers mentioned in this series, including Cigna, Anthem, and Blue Cross/ Blue Shield, did not respond to requests for comment from MindSite News. UnitedHealthcare responded but declined to comment.
Chris Bond, a spokesperson for America’s Health Insurance Plans (AHIP), an insurance trade association, provided this written statement:
“First, it’s important to note that health plans’ coverage decisions follow the latest medical guidelines on treatments and medical care that are proven to be safe and effective. Data on denials rarely take into account the overwhelming number of claims that are submitted from doctors that have extensive gaps in the accuracy and completeness of information provided, meaning health plans are regularly having to follow up to confirm correct billing and diagnostic codes or assess whether the care provided would have resulted in a different treatment plan.
“Second, health insurance is regulated unlike any other industry or product. States, employers, and federal regulators ultimately have an outsized and often final say on what benefits are included for consumers. So if a service is not included as part of coverage – as a result of an employer’s coverage policy or a state requirement – then it’s important to understand that distinction.
“Finally, every aspect of insurance is regulated or reviewed by state insurance commissioners AND federal regulators – from the cost of premiums, out-of-pockets and deductibles, to the number of providers and specialists considered in-network, to the use and speed of prior authorization in public programs. So there is a shared responsibility from a coverage and access standpoint among providers, drug makers and others to make this care easy to access too.”
“In what lifetime would somebody get a pre-approval for an ambulance?”
—BETH T, MOTHER OF GIGI
As of this writing, Gigi – now 19 – is in a residential treatment program in Dallas. Just prior to that admission, she attempted suicide and was transferred by ambulance to a psychiatric ward – a bill her mother is still waiting to be reimbursed for. “The insurance company is not paying for the ambulance ride, which was several thousand dollars, because they’re saying, well, we needed pre-approval,” her mother said. “I said: ʻIn what lifetime would somebody get a pre-approval for an ambulance? Like ‘I’m going to need an ambulance next week, let’s get the paperwork going for that,’ said no one, ever.”
Part 2 tomorrow: ‘A Front Row Seat to Desperation’: The Advocates Fighting to Remove Barriers to Eating Disorder Treatment.
Photo credit, image at top: Unsplash
Select References
Penwell TE, Bedard SP, Eyre R, Levinson CA. Eating Disorder Treatment Access in the United States: Perceived Inequities Among Treatment Seekers. Psychiatric Services. 2024;75(10):944-952.doi:10.1176/appi.ps.20230193
Timothy Walsh et al, A Systematic Review Comparing Atypical Anorexia Nervosa and Anorexia Nervosa, International Journal of Eating Disorders, August 2022
Bowman Family Foundation, Equitable Access to Mental Health and Substance Use Care: An Urgent Need, a Patient Experience Survey, July 2023, Conducted by NORC, University of Chicago
RTI International, Behavioral Health Parity – Pervasive Disparities in Access to In-Network Care Continue, Tami Mark, William Parish, April 17, 2024
Disparities in Access to Eating Disorders Treatment for Publicly-Insured Youth and Youth of Color, a Retrospective Cohort Study, Marissa Raymond-Flesch, UCSF corresponding author Ruby Moreno, Sara Buckelew et al, Journal of Eating Disorders, 2023
https://victusrecovery.com/wp-content/uploads/2025/05/Eating-Disorders-1024x576-1.png5761024Victus Counselinghttps://victusrecovery.com/wp-content/uploads/2024/09/Logo_VictusCounseling.pngVictus Counseling2025-05-12 04:35:422025-06-03 05:56:02The Deadly Cost of Eating Disorders: How Health Insurers Delay, Restrict and Deny Care
EDC Celebrates 25th Anniversary Advocating for Federal Funding to Support Eating Disorders Research, Prevention, and Provider Education
WASHINGTON, DC (May 9, 2025)- Yesterday, the Eating Disorders Coalition for Research, Policy, & Action (EDC) hosted its annual Advocacy Day in Washington, D.C. welcoming 140 advocates across 27 states and the District of Columbia. The day kicked off with energizing opening remarks from EDC Congressional Champion Senator Amy Klobuchar (D-MN) and wrapped up the afternoon with closing remarks from EDC Congressional Champion Senator Lisa Murkowski’s (R-AK) health staff. Advocates took part in 100 congressional meetings requesting their elected officials support the EDC’s Fiscal Year 2026 appropriations requests. Led by EDC Congressional Champions, Representatives Andrew Garbarino (R-NY-02), Judy Chu (D-CA-28), Brian Fitzpatrick (R-PA-01), Paul Tonko (D-NY-20), and Senator Amy Klobuchar (D-MN), EDC advocated for two requests within the U.S. Department of Health and Human Services:
$5 million for the Eating Disorders Center of Excellence within the Substance Abuse and Mental Health Services Administration to continue training clinicians in Screening, Brief Intervention, and Referral to Treatment for Eating Disorders (SBIRT-ED) model and develop and implement a public service announcement to raise awareness about eating disorders.
$750,000 for research grants within the Office on Women’s Health to focus on early detection of eating disorders in women and girls.
“Senator Klobuchar has been a long-time champion for people with eating disorders and their families,” said Jillian Lampert, PhD, MPH, RD, LD, FAED, Vice President of Strategy and Public Affairs at Accanto Health, EDC Board Member, and Minnesota constituent. “We appreciate her steadfast support and determined action that has made a difference in access to care. Recovery from an eating disorder is more possible in Minnesota and across the nation thanks to her efforts.” “I want to thank the Alaska Representative and Senators, particularly Senator Lisa Murkowski, for their understanding and advocacy regrading care discrepancies in our state and nation,” said Mina Hancock, EDC Young Leader Council Member and Alaska constituent. “It has been an amazing experience to be on Capitol Hill with such a powerful group of people. I truly cannot thank the EDC enough for the effort they put in to support those without a voice across the nation.”
“It was so inspiring to see so many folks from across the country come to DC to passionately advocate on behalf of the eating disorders community,” said Christine Peat, PhD, FAED, LD,EDC Board President. “It is with one united voice that we speak and in doing so we demonstrate to Congress that we are united in our demand that the federal government not leave eating disorders behind. We need these appropriations now more than even, and the EDC is privileged to do this work alongside such passionate advocates.”
The Eating Disorders Coalition for Research, Policy & Action is a federal advocacy organization based in Washington, D.C. The EDC advances the recognition of eating disorders as a public health priority throughout the United States.
Media Contact: Emily Rosenberg, er********@**********************on.org
SIOUX FALLS, S.D. (Dakota News Now) – 28.8 million Americans will have an eating disorder in their lifetime. It’s the number one cause of death among all mental health illnesses and affects lives emotionally, socially, and physically.
Victus Counseling owner and Clinical Therapist specializing in eating disorder treatment Faith Carlson explained the warning signs as, “You’re really gonna be looking at mood changes, at behavior changes, and you’re going to start to see a lot of isolation or rigidity. When I think of the medical side of it, labs will be off, GI, those will all be off. Then, when I think of the social side of it, they’re not engaging, there’s a lot of heightened anxiety or debility just because it’s such an overwhelming diagnosis.”
Stereotypically, it’s believed that only girls and young women experience eating disorders, but that’s not the case.
“It affects all ages. The youngest I’ve worked with is six years old. My oldest I’ve worked with is within their 70s. It’s men, it’s female, it’s all genders and there’s diversity. It impacts everybody,” Carlson said.
While an eating disorder doesn’t have a specific look, times like National Eating Disorder Awareness Week bring us an opportunity to educate ourselves on the topics.
“As a society, if we can recognize that we don’t need to comment on other people’s bodies, on other people’s foods, on other experiences or images… if you don’t know what to say, it’s best not to say anything,” Carlson said.
There are multiple resources available to help treat an eating disorder, but Faith also recommends identifying somebody in your life as a safe person. This individual can help you manage the struggles an eating disorder presents.
“A malnourished mind doesn’t know how to do all these critical steps. So, if you can identify one person who you feel like you can talk to to get the next steps, allowing that other person to get the footwork because their mind is fed and they can kind of multitask and do all that critical thinking,” said Carlson.
During National Eating Disorder Week, which is February 28 through March 2, Victus Counseling is lighting The Falls blue and green to draw awareness to this mental health illness.
For more information on eating disorders or for those seeking help, click here.
Eating Disorders Awareness Week shines a crucial light on a complex and often misunderstood group of mental health conditions.
Eating disorders, including anorexia nervosa, bulimia nervosa, and binge-eating disorder, impact millions of individuals across all demographics, causing significant physical and emotional distress.
Faith Carlson with Victus Recovery counsels people dealing with eating disorders. She knows that beyond the statistics lie real stories of struggle, hope, and the possibility of recovery.
Faith was here to help demystify eating disorders by helping us to recognize the signs and gain an understanding of the available resources to break down the stigma surrounding these illnesses and empower people to embark on a journey towards healing.
The BMI is a screening for body fatness that is frequently used to identify a person’s risk of disease. However, The CDC now warns against using the BMI as a means of diagnosing body fatness or health. One place where the BMI screening may in fact be missing the mark, is when it comes to diagnosing Anorexia Nervosa.
Faith Carlson is a Licensed Clinical Therapist and Eating Disorder Specialist.
She joined us to talk about atypical anorexia, a disease with the same symptoms and risks as Anorexia, just without the qualifying marker of a specifically low body weight or BMI. She also shared how that may lead to someone with a serious eating disorder to slip through the cracks in terms to getting the help they need. We do want to warn you that this conversation may include triggering language.
https://victusrecovery.com/wp-content/uploads/2024/11/Faith_Carlson_In_the_News.png654871Victus Counselinghttps://victusrecovery.com/wp-content/uploads/2024/09/Logo_VictusCounseling.pngVictus Counseling2024-07-15 22:26:072024-11-14 00:17:16You Don’t Have to be Thin to Have an Eating Disorder
Faith Carlson is a counselor with the Carroll Institute. She’s here today to explain how the pandemic may have triggered disordered eating among teens and adults.
















 Unpublished data shared with MindSite News by researchers at the EAT Lab showed that people with both private and public insurance faced major obstacles getting treatment for eating disorders. But on nearly all metrics, publicly insured patients had a harder time getting services and coverage. Specifically, they found:
Unpublished data shared with MindSite News by researchers at the EAT Lab showed that people with both private and public insurance faced major obstacles getting treatment for eating disorders. But on nearly all metrics, publicly insured patients had a harder time getting services and coverage. Specifically, they found: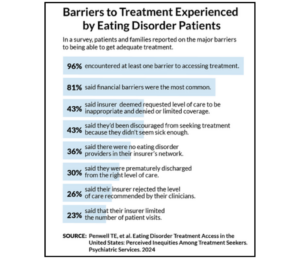 Survey: 96% of patients encounter obstacles to eating disorders treatment
Survey: 96% of patients encounter obstacles to eating disorders treatment